| |
Highlights
Burns need to be accurately diagnosed for proper treatment and healing. This is difficult because it can take up to a week to accurately assess the depth of a burn. Researchers have developed a tool to assess burn depth quicker. The researchers isolated the proteins in burn blister fluid and used a variety of techniques to determine the individual proteins found in each blister fluid sample. After analysis, the researchers looked for patterns between proteins and burn characteristics. The researchers found that certain proteins were related to burn depth and could be used as predictors of burn depth. Most of these proteins are involved in immune system function such as inflammation or protection while others are intracellular and extracellular matrix proteins. The researchers are creating a protein profile to indicate burn depth, which would allow clinicians to make faster and better decisions about burn treatment.
Did you know that the skin is the largest organ in your body? Skin is so important because it’s an airtight and watertight barrier that keeps everything that’s supposed to be inside the body inside, and everything that’s supposed to stay outside of the body outside. It also helps regulate temperature and fight infection, and it’s responsible for our sense of touch.
What we think of as skin is actually three layers of protective coating around the body. The
epidermis
is the outermost layer of skin that usually comes in contact with the outside world. The cells of the epidermis are packed very closely together so no moisture can get in or out. The epidermis is a very thin layer, about the thickness of a human hair. In fact, if you get a very minor scratch and it draws blood you have gone right through the epidermis and into the next layer of skin, the
dermis.
The dermis is the middle layer of skin and lies beneath the epidermis. This layer is 30 to 40 times thicker than the epidermis and is still only about 0.1 inches deep beyond the outer layer of the skin. The depth of the dermis depends on the location on the body and the person’s gender. Inside the dermis lies blood vessels, nerves, glands, and the base of hair follicles.
Underneath the dermis is the final layer of skin called the
subcutis
or hypodermis. The subcutis is made of fat and connective tissue. It contains larger blood vessels and nerves and helps regulate body temperature. The depth of the subcutis varies by area of the body, and by age, gender, and weight.
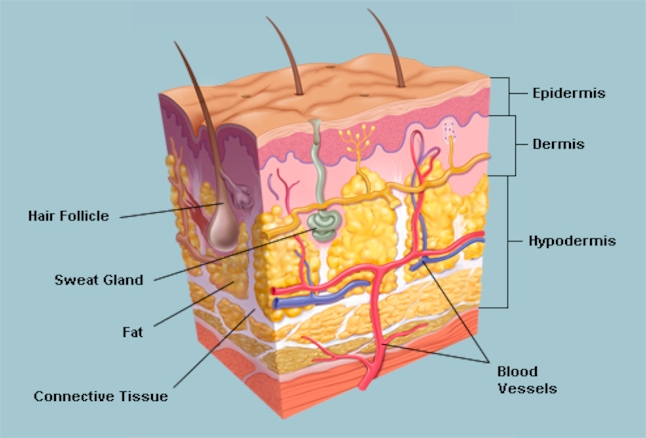
Figure 1. Layers of human skin
[Source:https://www.webmd.com/skin-problems-and-treatments/picture-of-the-skin#1]
Given the layers of skin surrounding our bodies, it makes sense that there are also many different ways to injure the skin. One particularly painful—and potentially dangerous—way of damaging the skin is through burns.
Burns occur when the skin comes in contact with an irritant or energy source, which destroys the skin cells. There are different types of irritants or energy, and so there are also different types of burns:
chemical burns
(from harsh chemicals),
electrical burns
(from electricity),
radiation burns
(exposure to radiation like a sunburn), and
thermal burns
from contact with hot liquids, objects or fire. By far the most common type of burn in children are thermal burns that occur from spilling hot beverages or getting too close to a hot object like a stove or an iron.
The severity of a burn varies based on the size of the burned area and the depth of the burn. Burns are generally categorized by the layer of skin affected:
Superficial (first degree) burns
affect only the epidermis,
partial thickness (second degree) burns
affect the epidermis and the dermis, and
full thickness (third degree) burns
affect the epidermis, dermis, and subdermis. Since the dermis and subdermis can vary greatly in depth, it can often be difficult to tell exactly how deep a burn goes.
Superficial burns are the typical types of burns many people have experienced. There are no blisters, just some pain and redness, and it usually heals within a week without leaving a scar. Partial thickness burns cause lots of pain and blistering and they are more variable in scarring and healing time, depending on how deep into the dermis the burn went. Some partial thickness burns can heal within two to three weeks without leaving a scar while others can take more than three weeks, leave a scar, and may even require a skin replacement known as a
skin graft
in order to fully heal. Full thickness burns usually don’t cause pain because the nerve endings that transmit pain are damaged. The damaged skin looks shiny and white. Full thickness burns often require a skin graft and can take three to six weeks or longer to heal.
In addition to severity, burns also differ in their size. Burn size is usually measured as a proportion of
total body surface area.
Burns that are less than 5% of total body surface area are considered less severe, while burns that affect more than 5% of total body surface area are considered more severe.
If you are burned, the best thing to do is to immediately run cool water over the burn for at least twenty minutes to cool the skin and prevent further burning. Over-the-counter medicines like acetaminophen (Tylenol) can be used to help with pain. Burns require medical attention if they are white in appearance (indicating they are quite deep), or located on sensitive areas of the body, such as the face, hands, feet, groin, or
perineum.
Medical attention should be sought for all burns in children.
Figure 2. Initial treatment of burns
For burns that require medical attention, treatment depends on a doctor’s assessment of how deep the burn goes and how much total body surface area has been affected. Burns need to be well cleaned to prevent infection, a process known as
debridement.
Depending on the situation, debridement can take place with minimal pain control or it may require general anesthesia. If a large amount of the body has been affected, antibiotic treatment is often required and can range from antibiotic creams to pills to intravenous medications. In more severe cases, a skin graft might be required. A skin graft is a procedure where replacement skin, oftentimes from somewhere else on the patient’s body, is placed over the burned area.
Up until now we have been describing burns and their treatments for everyone, adults and children alike. But children with severe burns can face especially long roads to recovery. This is because the
scar tissue
that forms is not mobile and elastic like the rest of our skin. It is actually quite rigid and doesn’t stretch, which can lead to difficult problems for growing children. Severe burns in children may require follow-up surgeries for many years, until the child stops growing, to replace skin grafts and ensure joint mobility.
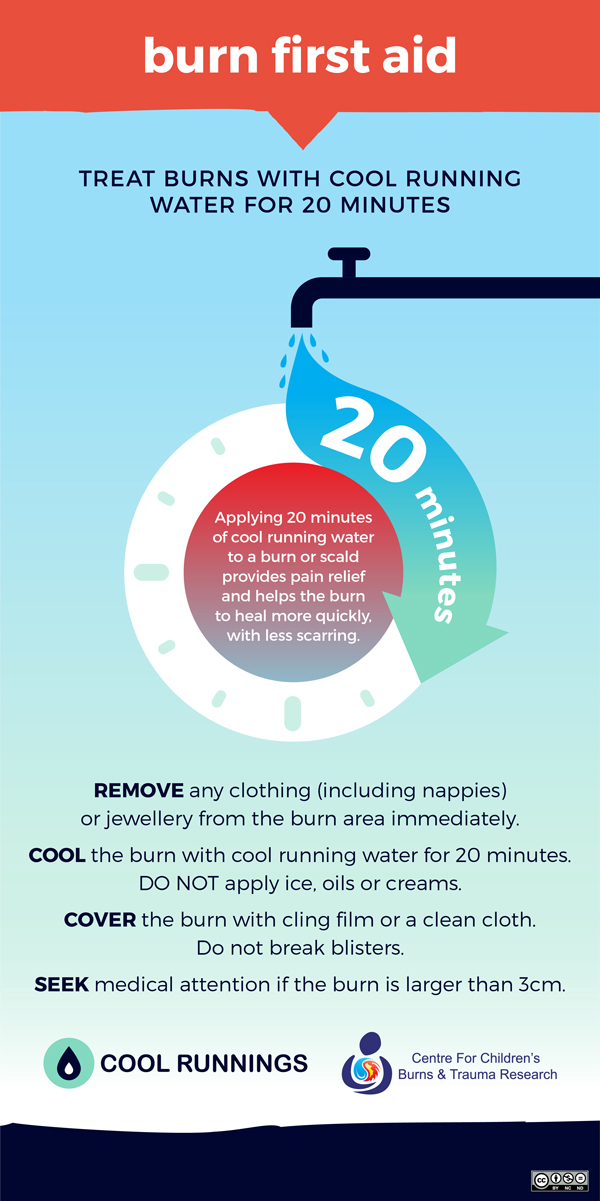
Figure 3. Burn first aid
When a burn needs medical attention, doctors who specialize in burns assess the severity of a burn based on its depth, total body surface area affected, and likelihood of healing and scarring. Based on this assessment, clinicians will make a recommendation for continued treatment. They need to work fast, because the quicker burns are appropriately treated, the more likely they are to heal properly. This is complicated by the fact that it can take up to a full week in some cases to accurately assess the depth of a burn.
What if there was a way to assess a burn more quickly? That’s the goal of research conducted by Dr. Tony Parker and Associate Professor Leila Cuttle at Queensland University of Technology in Brisbane, Australia. Dr. Parker is a research scientist specializing in the cutting-edge technology of protein analysis, and Associate Professor Cuttle is a research scientist specializing in burn treatment. Dr. Parker and Associate Professor Cuttle teamed up to figure out if they could find a better diagnostic tool for burns based on the protein profile of burn blister fluid.
Until Dr. Parker and Associate Professor Cuttle began their research, fluid from burn blisters was usually discarded as part of routine wound cleaning. The researchers thought there might be information in that fluid that would be useful for burn treatment, so they asked participating clinicians to save the fluid for them instead of discarding it. Patients and their families were told about the research and consented to collect the burn fluid. In addition, the researchers received permission to collect clinical information about the cause, severity, and treatment of the burn, as well as information about the patient’s age, gender, and time since the burn injury. In total they collected samples from 87 pediatric patients treated for burns. The researchers used this information to draw connections between the protein profiles of different burns and the patient’s clinical outcomes.
Initially, the researchers isolated the proteins in the samples of blister fluid using a technique called
gel electrophoresis.
Gel electrophoresis separates proteins based on their size by using an electric current to push them through a porous gel material. The smaller the protein, the farther it will move through the gel. Using gel electrophoresis, the researchers identified eight important proteins to study further.
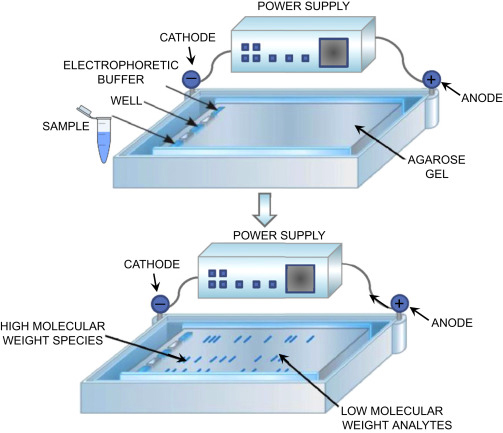
Figure 4. Gel electrophoresis
[Source: https://www.sciencedirect.com/topics/neuroscience/gel-electrophoresis]
Next, the researchers wanted more information about the proteins they identified. Proteins are large molecules made up of smaller pieces called amino acids. There are twenty amino acids that form the hundreds of thousands of proteins in the world, and the researchers wanted to know the make-up and ordering of those amino acids for each isolated protein. To do this, the proteins were mixed with an
enzyme
called trypsin, which cut the larger proteins into smaller pieces called
peptides,
which were between about six and twenty amino acids long.
These protein pieces (peptides) were then analyzed with a technique known as sequential window acquisition of all theoretical mass spectra or
SWATH-MS
for short. SWATH-MS combines several analytical techniques including
liquid chromatography
and
mass spectrometry.
Liquid chromatography separates the peptides dissolved in solution, and mass spectrometry identifies peptides based on their mass. In this way, the researchers could identify the peptides with SWATH-MS to determine which proteins were in each blister fluid sample. This test not only detected each of the proteins previously identified during gel electrophoresis, it also identified lots of other proteins the researchers wanted to know more about.
At the end of the SWATH-MS analysis, the researchers had a digital copy of the individual proteins found in the blister fluid and a picture of how much of each protein was in each sample. Most of the proteins identified are involved in
immune system
function such as
inflammation
or protection. Once all the blister fluid proteins had been analyzed, the researchers looked for patterns between proteins and burn characteristics.
Some of the variables the researchers considered were:
- How the burn occurred
- The clinician’s assessment of the depth of the burn
- Total body surface area of the burn
- How long the burn took to heal
- Any needs for scar management therapy or skin grafting
- Age, gender, and other demographic information
The researchers compared the variables above with the abundance of certain proteins in blister fluid. They found that certain proteins were related to clinical outcomes of pediatric burns, and therefore they could be used as predictors of those outcomes. For example, subunits of the protein
hemoglobin,
which carries oxygen in the bloodstream, were found in higher concentrations when the burn depth was greater. Combined with other proteins involved in inflammation, the researchers hope to create a profile that would indicate greater or lesser burn depth, allowing clinicians to make faster and better decisions about burn treatment.
However, Drs. Parker and Cuttle caution that there is still more work to be done before blister fluid can be used to predict clinical outcomes. The goal of the experiments described here was to identify any proteins that might be related to different clinical outcomes. Now that the researchers have identified potential protein targets, they need to further test these proteins to ensure that they’ve really found the best ones.
Additionally, the experiments described here were done using a relatively small number of samples from pediatric patients. In future experiments, Drs. Parker and Cuttle plan to increase the number of participating patients and include samples from adults. “We assume that children and adult burns would be similar,” explained Associate Professor Cuttle, “but we have to test that hypothesis too.”
There are many more experiments that could be done with this data. For example, the researchers want to compare burn fluid samples of the same burn over time to see how the burn protein profiles change. They also want to compare fluid samples from burns on different parts of the same patient’s body.
As burn researchers, both Drs. Parker and Cuttle emphasize the importance of burn prevention and proper burn first aid. “The most common burns in children are due to scalds from hot drinks or hot food,” explained Associate Professor Cuttle, “so it’s really important to take precautions when making or drinking hot beverages and cooking.” Dr. Cuttle continues, “And if you do get burned, the most important thing is to run cool water over the burn for 20 minutes.”
Dr. Tony Parker is Deputy Leader of the Tissue Repair and Translational Physiology Program and Senior Lecturer within the School of Biomedical Sciences at Queensland University of Technology in Brisbane, Australia. Much of his research focuses on tissue injury and recovery using cutting-edge analytical techniques. Dr. Parker started his scientific career as an adult. After graduating from high school, Dr. Parker worked in the construction industry for 13 years before deciding to change careers and pursue a college degree. When he works with students, Dr. Parker always emphasizes the many different pathways that can lead to a career in the sciences. “You don’t have to be the smartest person in the room if you’re willing to work hard.” When not in the laboratory, Dr. Parker enjoys boating, reading about history, politics, and philosophy, and spending time with his family.
Leila Cuttle is Associate Professor, Leader of the Tissue Repair and Translational Physiology Program and a Senior Research Scientist at Queensland University of Technology in Brisbane, Australia where she works to improve the care of pediatric burn patients. In addition to the research described here, Associate Professor Cuttle focuses on engineering skin tissue to be used in skin grafts and teaching tissue engineering to students. When not in the laboratory, Associate Professor Cuttle enjoys cooking, drinking different teas, and going out to new restaurants.
For More Information:
- Zang, T. et al. 2019. “Characterization of the blister fluid proteome for pediatric burn classification.” Journal of Proteome Research, 18(1): 69-85.
- Zang, T. et al. 2016. “The biochemistry of blister fluid from pediatric burn injuries: proteomics and metabolomics aspects.” Expert Review Proteomics, 13(1): 35-53.
- Zang, T. et al. 2016. “Mass spectrometry based data of the blister fluid proteome of paediatric burn patients.” Data in Brief, 8:1099-1110.
- Zang, T. et al. 2016. “The blister fluid proteome of paediatric burns.” Journal of Proteomics, 146: 122-132.
- Tanzer, C. et al. 2015. “Evaluation of haemoglobin in blister fluid as an indicator paediatric burn wound depth.” Burns, 41: 1114-1121.
To Learn More:
- Centers for Disease Control and Prevention. https://www.cdc.gov/safechild/burns/index.html
- American Burn Association. http://ameriburn.org/prevention/prevention-resources/
- Shriners Hospitals for Children. https://www.shrinershospitalsforchildren.org/shc/beburnaware
- World Health Organization. https://www.who.int/violence_injury_prevention/other_injury/burns/en/
- Phoenix Society for Burn Survivors. https://www.phoenix-society.org/
Written by Rebecca Kranz with Andrea Gwosdow, PhD at www.gwosdow.com
HOME | ABOUT | ARCHIVES | TEACHERS | LINKS | CONTACT
All content on this site is © Massachusetts
Society for Medical Research or others. Please read our copyright
statement — it is important. |
|
|

Team photo from left to right: Dr. Tuo Zang, Dr. Daniel Broszczak
Dr. Catherine Tanzer, Associate Professor Leila Cuttle, Dr. James Broadbent, Dr. Tony Parker

Dr. Tony Parker

Associate Professor Leila Cuttle
Sign Up for our Monthly Announcement!
...or  subscribe to all of our stories! subscribe to all of our stories!

What A Year! is a project of the Massachusetts
Society for Medical Research.
|
|
