05/10 - Recovering from Recession - MSMR: What A Year!
05.10 Recovering from Recession
Recovering from Recession With Far Less Pain
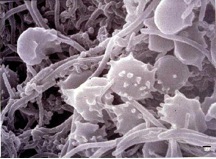
Figure 1: Dental plaque, scanning electron micrograph illustrating the diversity of microbes in plaque.
The National Institute of Dental and Craniofacial Research
estimates that about 80% of American adults have some type of
periodontal disease, more commonly known as gum disease.
Periodontal disease
can range from minor inflammation along the gum-line to severe damage to gum tissue and facial bones. It is caused by bacteria that create a colorless film on the teeth known as
plaque
.
Plaque also causes
dental caries
,
more commonly known as
cavities.
In order to remove plaque from our teeth, we are told to brush our teeth after each meal and floss daily. Plaque that remains on the teeth for a prolonged period of time hardens into tartar, also known as
calculus,
that can only be removed by a dental professional. If you've been to the dentist recently, you may remember some scraping and sanding to get rid of this tartar buildup. We are also told to see a dentist twice a year. Plaque and tartar harbor bacteria that cause inflammation in the gums. This inflammation is the milder type of periodontal disease known as gingivitis . The symptoms of
gingivitis
include red, swollen gums that bleed easily and can be tender. Gingivitis can usually be reversed with daily oral hygiene and regular visits to the dentist.
However, if untreated, gingivitis can lead to further inflammation around the teeth. This allows the bacteria to spread below the gum line. The bacteria produce toxins that irritate the gums and cause the gums to pull away from the teeth, creating pockets where the bacteria can thrive. The toxins also stimulate a response of the
immune system
that cause the gum tissue and bones that support the teeth to break down. This condition is known as
periodontitis.
Over years, periodontitis can eventually lead to tooth loss as the bone and gum tissues that support the teeth disappear. One of the first signs of periodontitis is recession of the
gum line
where the gum tissue surrounding the teeth erodes, exposing the teeth roots that were previously covered. Not only is recession not aesthetically pleasing, it causes teeth to be more sensitive to hot and cold and more susceptible to cavities. Even people who do not have cavities in their teeth may get cavities in their roots as a result of gum recession because teeth roots are not protected by enamel-like teeth.
Figure 2 - Moderate to severe recession before treatment
Figure 3: Same patient with final healing after grafting with restoration of normal gingival contours and also the placement of porcelain veneers with gold restorations in the posterior segments
The Old Way
Periodontitis can be reversed using a variety of remedies including professional deep cleanings to remove tartar below the gum line and antibiotics. Gum recession associated with periodontitis can be treated with surgery known as a
tissue graft
that replaces the lost gum tissue with tissue taken from elsewhere on the body. Generally an oral tissue graft will use tissue from the roof of the patient's mouth, known as the
palate.
This palatal tissue will then grow and cover the exposed roots where tissue was lost. The most common side effects of such surgery are bleeding, pain, and swelling. These complications stem from the initial step of removing a sample of palatal tissue from the roof of the patient's mouth rather than from the grafting procedure itself.
The pain and swelling associated with oral tissue grafting surgery cause many patients to reject such treatment and, instead, face potential tooth loss in the future. For many years, there were no other options for treating gum recession. Recently, however, Dr. Terrence Griffin of the Tufts University School of Dental Medicine has developed a grafting procedure without the use of palatal tissue that is comparatively pain-free.
”We used to think,“ remarked Dr. Griffin, "that palatal tissue would completely regenerate without scarring." This is what made the use of palatal tissue for oral grafts so appealing. However, we now know that palatal tissue only somewhat regenerates, so that taking palatal tissue for grafting surgery actually causes a thinning of the palate. This is why the surgery is often so painful.
The New Way - Less Pain and Better Results
Dr. Griffin wanted to develop a technique for oral grafting surgery that would avoid the painful process of removing palatal tissue. He hypothesized that
platelets
might be a natural alternative to palatal tissue because of their role in the healing process. Platelets are a type of immune cell that rush to the wound site as the initial step of an immune response. For example, when you cut yourself, platelets create a clot at the wound to stop bleeding. Platelets will also release
growth factors
at the wound to stimulate new blood vessel growth and
collagen
synthesis. Collagen is the most abundant protein in
connective tissue.
A wound will heal as collagen is synthesized to cover the affected site.
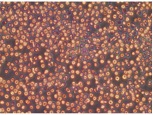
Figure 4: Whole blood - Platelets are very small white dots.
Platelets are found in the part of the blood known as
plasma.
Plasma makes up over half of the volume of blood and can be isolated by spinning a sample of blood around rapidly in a machine called a
centrifuge.
This causes all the blood cells contained in the blood to fall to the bottom, leaving the plasma, a yellow liquid, at the top. Plasma is mostly water along with platelets, dissolved proteins, salts, sugars, and minerals like calcium, sodium, magnesium, and potassium. Platelets, being very small and light, congregate in the lower levels of the plasma just above the red blood cells and white blood cells which are heavier.
Figure 5: Platelet concentrate - Note the presence of many more platelets (small white dots).
To test his idea of using platelets in grafting surgery, Dr. Griffin conducted a pilot study where he took blood samples of several patients prior to their grafting surgery. The platelets were concentrated in the plasma, creating a substance known as platelet-rich plasma, or PRP. Dr. Griffin placed the PRP on a collagen sponge, which he used instead of palatal tissue for patients involved in the study. He found that the patients who underwent surgery with PRP had quicker healing and better aesthetic results than patients who had undergone the more traditional procedure using palatal tissue. The reason that Dr. Griffin's patients had better aesthetic results is because palatal tissue is tougher and whiter than other gum tissues. When it is grafted, palatal tissue is bumpier and whiter than normal gum tissue, making a less pleasing looking result. The procedure using PRP, however, stimulates the growth of naturally-occurring gum tissues so the result is a more natural looking gum line.
A Promising Control Study 3-Year Follow-up
With the promising results of his pilot study, Dr. Griffin conducted a control study of fifteen patients where he used palatal tissue on one side of the mouth and a PRP collagen sponge on the other. Both grafting procedures had similar root coverage; however, doctors consistently chose the PRP collagen sponge method as having better aesthetic results. Additionally, patients reported less pain and swelling on the side of their mouth where the PRP collagen sponge had been used. The results of the control study demonstrated further promise for this new technique.
However, Dr. Griffin was still concerned because if any of the PRP or collagen sponge were exposed, it would disintegrate within 24 hours. In order to stabilize the sponge, Dr. Griffin placed the collagen sponge in a collagen membrane that is more resistant to the movements in the mouth. He then placed spacers in the collagen membrane to provide more structure.
In a recent follow-up study, Dr. Griffin looked at the mouths of patients 3 years after they had undergone the grafting procedure using the PRP collagen membrane. He found new bone growth in the affected sites, and the results of the procedure three years post-operation were better than the results after 3 months!
Currently, Dr. Griffin and one of his associates, Dr. Wai Cheung, are the only
periodontists
in the country who can perform the grafting surgery using the PRP collagen sponge. The next project for Dr. Griffin is to create an assembly kit for other periodontists to use. This kit would contain directions for preparation of PRP as well as collagen sponge spacers and the collagen membrane. "There are clear advantages to this technique," Dr. Griffin explained. First, with palatal tissue you can only obtain enough graft material for two to four teeth at a time. On the other hand, it is possible to produce enough PRP to graft the entire mouth with only a few small tubes of blood. Second, this procedure is less painful. Dr. Griffin hopes that his new, pain-free procedure will encourage patients to seek more treatment for gum recession so they do not lose their teeth. "Instead of leaving (the dentist's office) with stitches in your mouth," remarked Dr. Griffin, "patients leave with a small temporary band-aid on their arm."
In order to determine why this technique is so effective, a study is currently underway to examine the differences in gum tissue grafts after surgical procedures using an animal model. The procedures included in the study will include traditional palatal tissue grafts, grafts using PRP and a collagen sponge, and grafts using PRP, a collagen sponge, and a collagen membrane. From this study, Dr. Griffin hopes to determine how the different grafts attach to the roots, which procedures produce bone, and which procedures result in functional orientation of the
ligaments.
This will enable Dr. Griffin to understand the mechanisms of tissue repair that result from the different grafting procedures.
Dr. Terrence Griffin is a practicing periodontologist in Boston and the Chair and Director of Postdoctoral
Periodontology at Tufts University School of Dental Medicine. Dr. Griffin was always interested in science and medicine and chose dentistry because he did not want to deal with life-or-death procedures. He became a periodontist because he enjoyed the surgery aspect of dentistry. When not teaching or practicing dental medicine, Dr. Griffin can often be found on the golf course. He is an avid golfer who has golfed all over the world. Once a year, he meets 23 other doctors from around the United States to go golfing for a week in Ireland. Dr. Griffin also enjoys spending time with his family.
To learn more:
Cheung, W. and T. Griffin. (2004). "A Comparative Study of Root Coverage with Connective Tissue and Platelet Concentrate Grafts: 8-Months Results." Journal of Periodontology, 75(12): 1678-1687.
Griffin, T. and W. Cheung. (2009). "Guided Tissue Regeneration-Based Root Coverage with a Platelet Concentrate Graft: A 3-Year Follow-Up Case Series." Journal of Periodontology, 80(7): 1192-1199.
Griffin, T. et al. (2006). "Postoperative Complications Following Gingival Augmentation Procedures." Journal of Periodontology ,77(12): 2070-2079.
Kassab, MM, Cohen, RE. The etiology and prevalence of gingival recession. Journal of the American Dental Association 2003;134:220-225.
Kontovazainitis G, Griffin TJ, Cheung WS. Treatment of gingival recession using platelet concentrate with a bioabsorbable membrane and a coronally advanced flap: A report of two cases. International Journal of Periodontics and Restorative Dent 2008;28:301-307.
Griffin TJ, Cheung WS. The treatment of gingival recession with a platelet concentrate graft A report of two cases. International Journal of Periodontics and Restorative Dentistry 2004;24:589-595.