Approximately 5 million Americans
are living with heart failure and nearly 600,000 people die
of heart failure every year in this country. Heart failure,
or cardiac failure, means that the heart isn’t pumping
as well as it should. As a result there is reduced blood flow
to the heart. The heart needs to pump blood in order to deliver
oxygen- and nutrient-rich blood to all cells in the body. When
the cells are nourished properly, the body can function normally.
When the cells do not have enough blood, such as with heart
failure, a person will feel tired, get short of breath easily
and everyday activities such as walking, climbing stairs or
carrying groceries become hard to do.
Let’s discuss the
heart in more detail. The heart cannot sustain itself for long
with low blood flow, and will die when exposed to low blood flow
for an extended period of time. The condition of reduced blood
flow to the heart is called ischemia.
When the body senses low blood flow, the heart tries to compensate
by increasing blood flow. It can be increased two ways: by having
your heart beat more times a minute (increasing your heart rate),
or by increasing the force of each beat or contraction. These
mechanisms can work for a while, but usually they cause the heart
to enlarge, or hypertrophy. An enlarged heart can result from
numerous body conditions. Two of the leading ones are high blood
pressure and obesity. The hearts of patients with high blood
pressure or obesity will eventually hypertrophy because of the
increased blood pressure needed to pump blood around the body.
In a hypertrophied heart, heart cells will die. When they die,
they are replaced by scar tissue that cannot contract like normal
heart cells. As a result, the heart muscle becomes stiffer and
stiffer as scar tissue builds up over time. Eventually the heart
will not be able to contract properly and the patient will experience
cardiac failure, and even a heart attack.
Once a heart has hypertrophied it may be months, years, or decades
before cardiac failure ensues, but no matter how long it takes,
cardiac failure is the next step after hypertrophy.
What can we do to protect a hypertrophied heart?
Almost three decades ago, a technique called preconditioning
was proposed to protect hypertrophied hearts from cardiac failure.
In the same way that you build up strength as you exercise over
time, the heart muscle builds up resistance to ischemia (reduced
blood flow). Hearts that recover from ischemia appeared to be
more resistant to further ischemia, so the idea was to condition
the heart to adapt to ischemia and thus survive for longer periods
of time. In the decades since the idea was first proposed, much
research has gone into what makes preconditioned hearts able
to withstand long periods of ischemia.
Dr. Karyn Butler, Associate Professor of
Surgery in the Division of Trauma and Critical Care at the University
of Cincinnati, has recently made a significant breakthrough in
identifying a specific mechanism associated with preventing ischemia
in hypertrophied hearts. In particular, she investigated the
JAK-STAT pathway. JAK-STAT stands for Janus kinase (JAK)-Signal
Transducers and Activators of Transcription (STAT). The details
of this intimidating-sounding pathway are beyond this What A
Year! story: for now what we need to know is that the pathway
has been identified in many different cardiac functions or diseases.
In particular, studies have shown that parts of the JAK-STAT
pathways are activated during ischemia.
Dr. Butler is both a surgeon and a researcher
specializing in cardiac biology. She has been interested in the
preconditioning of hypertrophied hearts for many years. She wanted
to know what specific proteins were involved in the increased
resistance to ischemia in hypertrophied hearts. One goal at some
time in the future is to develop a drug that might assist the
JAK-STAT pathway in protecting people’s hearts.
To study ischemic preconditioning,
Dr. Butler first needed an animal model of an enlarged heart.
She began by feeding rats a high-salt diet for two weeks to induce
high blood pressure, and eventually, cardiac hypertrophy developed
in these animals. Once hypertrophied, the hearts were studied
ex vivo, or outside of the body. In order to study the function
of the heart, Dr. Butler uses a machine that mimics the cardiovascular
system, pumping a solution through the heart to keep it functioning.
Using this system (shown above), Dr. Butler can simulate ischemia
by stopping the flow of solution to the heart.
Courtesy
of Garret Gross, PhD
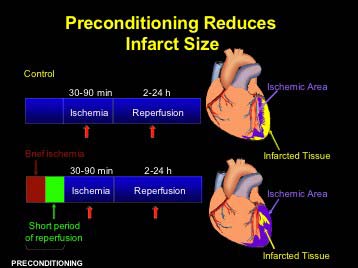
To test the idea of preconditioning, Dr.
Butler stopped the flow of solution briefly (5 minutes) prior
to stopping it for a longer period (30 minutes). After this preconditioning,
the flow to the heart was restored. Dr. Butler then examined
the post-ischemia hypertrophied heart function and the heart
tissue itself. She
compared it to post-ischemia hypertrophied hearts that had not
been preconditioned (control hearts). Dr. Butler found that rats
whose hearts were preconditioned had less infarcted (= dead)
tissue compared with control hearts, as shown in the figure above.
[Note: reperfusion is the return of blood flow to the heart after
ischemia.]
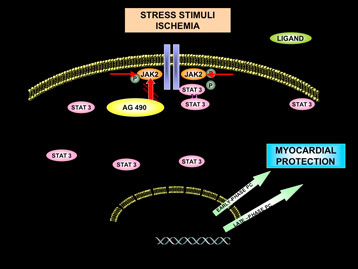
Next, Dr. Butler tried to find the protein that had been activated
by the hypertrophied heart and that could therefore be responsible
for reducing heart damage. These experiments helped Dr. Butler
identify a protein in the intracellular signaling JAK-STAT pathway,
shown in the figure below. She and her team identified the protein
called STAT3, as being activated in hypertrophied hearts after
preconditioning. In contrast, STAT3 was not activated in the
hearts from control animals. She identified this as an important
step in the mechanism that leads to preventing damage from ischemia,
called ischemia resistance.
The next step was for Dr. Butler to
study animals without the STAT3 protein, called STAT3 “knock-out” animals.
By observing how hypertrophied hearts of animals without the
STAT3 protein fare during ischemia, Dr. Butler hoped to gain
broader insight into the particular role of this protein in strengthening
hypertrophied hearts.
“This is an important step along the way,” said Dr.
Butler, “but there are many more steps left before we can
fully identify this complicated pathway that is crucial to heart
function.” Dr. Butler demonstrated that STAT3 was a key
player in preconditioning by using knock-out animals as well
as animals given a drug to inhibit the JAK-STAT pathway. Both
of these animals responded just like controls – they could
not deal with ischemia and had larger areas of infarcted tissue.
In contrast, preconditioned animals responded to ischemia by
increasing STAT3 protein, and decreasing the size of damaged
cells. As a result, preconditioning was shown to improve heart
function.
How Will This Help?
Dr. Butler’s research has identified
a key component of the pathway. In addition, she has shown that
preconditioning the heart is helpful in protecting hypertrophied
hearts from further damage. This practice of preconditioning
may be used in hospitals during heart operations such as cardiac
bypass surgery. It is hoped that one day a drug such as an activator
of the JAK-STAT pathway can be used to precondition hearts as
a way of protecting them.
Dr. Karyn Butler is an Associate Professor
of Surgery at the University of Cincinnati specializing in trauma
and critical care. She splits her time between performing surgeries
and doing research. She notes that her career took a different
path than she imagined as a kid. In high school, Dr. Butler had
planned on becoming a veterinarian, but sickness in her family
changed her mind and she decided to go to medical school. After
medical school, residency and specialized training in trauma
and critical care, she was offered a job at the University of
Colorado where she was exposed to cardiovascular research. “I absolutely
loved research,” said Dr. Butler. “I knew this is
what I wanted to do. I love combining research and clinical medicine
as a career!”
Karyn Butler, Alice Huang, and
Judith Gwathmey. "AT1-receptor
blockade enhances ischemic preconditioning in hypertrophied
rat myocardium." American Journal of Physiology.
Heart and Circulatory Physiology (1999): 2482-2487.
Karyn Butler, Lynn Huffman, Sheryl
Koch, Harvey Hahn, and Judith Gwathmey. "STAT-3 activation
is necessary for ischemic preconditioning in hypertrophied
myocardium." American
Journal of Physiology. Heart and Circulatory Physiology 291(2006):
797-803
Lynn Huffman,
Sheryl Koch, and Karyn Butler. "Coronary effluent
from a preconditioned heart activates the JAK-STAT pathway
and induces cardioprotection in a donor heart." American Journal of Physiology.
Heart and Circulatory Physiology 294(2007): In press.
Bolli, Roberto, et al. "Myocardial
Protection at a Crossroads: The Need for Translation Into
Clinical Therapy." Circulation
Research 95(2004): 125-134.
Roberto Bolli, Dawn Buddhadeb,
and Yu-Ting Xuan. "Role
of the JAK-STAT Pathway in Protection Against Myocardial
Ischemia/Reperfusion Injury." Trends in Cardiovascular
Medicine 13(2002): 72-79.
Meldrum, Daniel. "Mechanisms
of Cardiac Preconditioning: Ten Years after the Discovery
of Ischemic Preconditioning." Journal
of Surgical Research 73(1997): 1-13.

 To study ischemic preconditioning,
Dr. Butler first needed an animal model of an enlarged heart.
She began by feeding rats a high-salt diet for two weeks to induce
high blood pressure, and eventually, cardiac hypertrophy developed
in these animals. Once hypertrophied, the hearts were studied
ex vivo, or outside of the body. In order to study the function
of the heart, Dr. Butler uses a machine that mimics the cardiovascular
system, pumping a solution through the heart to keep it functioning.
Using this system (shown above), Dr. Butler can simulate ischemia
by stopping the flow of solution to the heart.
To study ischemic preconditioning,
Dr. Butler first needed an animal model of an enlarged heart.
She began by feeding rats a high-salt diet for two weeks to induce
high blood pressure, and eventually, cardiac hypertrophy developed
in these animals. Once hypertrophied, the hearts were studied
ex vivo, or outside of the body. In order to study the function
of the heart, Dr. Butler uses a machine that mimics the cardiovascular
system, pumping a solution through the heart to keep it functioning.
Using this system (shown above), Dr. Butler can simulate ischemia
by stopping the flow of solution to the heart.