Imagine carrying an infectious disease affecting nearly one-third the global population and not even knowing it. Since you dont know youre infected, you then infect ten to fifteen other people, each year! They probably wont know theyre infected either, so theyll spread the disease in the same way. Before you know it, two billion people will be carrying the infection.
If the infection never caused any harm, it wouldnt matter that so many people had it. But about 10 percent of those two billion people will develop symptoms of this disease, tuberculosis, caused by the bacteria Mycobacterium tuberculosis. Most infections of tuberculosis occur in developing countries, particularly in the poorest and most rural areas with very little access to medical care. Once a person is infected with the M. tuberculosis bacteria, the body forms a hard shell around the bacterial colonies to contain them. As long as the bacteria are contained, the person does not experience any symptoms, but can still infect other people. This is known as "latent" tuberculosis infection. If the immune system is not strong enough to contain the colonies, however, eventually bacteria will escape into the bloodstream, where they will travel to different organs and cause severe damage. This is when people experience symptoms of tuberculosis disease. Tuberculosis usually affects the lungs, but the symptoms depend on where in the body the bacteria are multiplying.
Tuberculosis is treatable through a regimen of antibiotics. Why then, do several million people die annually from the disease? About half of the deaths from tuberculosis result from complications with HIV/AIDS. People with HIV/AIDS are 20 to 40 times more likely to die of tuberculosis than people not affected by the disease. Mostly, though, tuberculosis is so deadly because it is hard to prevent widening infection when there are so many people out there spreading the bacteria who dont know they are infected.
Catch It Early
Part of the solution to this problem, then, is to find people who are infected and treat them with antibiotics so they cant continue to spread the disease. However, this is more easily said than done. First, the populations most severely affected by tuberculosis dont have good access to medical care. They will not seek out treatment unless they are already infected, if then. So, those carrying the disease will not be treated. In order to identify latent tuberculosis in these populations, medical providers must come to the communities.
Once there, though, medical providers must have a way to easily test for tuberculosis. In the United States, the most common tuberculosis test is a skin test. For this test, a small amount of fluid containing M. tuberculosis proteins is injected into your forearm. If you have ever been exposed to the bacteria, they will react with the proteins and form a red bump over the injection site within two days. If the skin test appears positive, an x-ray, called a chest radiograph, can be used to determine whether the infection is latent or active. These technologies, however, cannot be applied in the places where they are most needed. In order for a test to be applicable in poor, rural areas, it needs to be cheap, portable, and fast. Skin tests take several days to develop, which require that the patients come back a second time. Chest x-ray machines are expensive, require extensive training and, as you might imagine, are not portable.
Several tests are used in the developing world, but they face significant challenges. For example, tuberculosis is typically detected through a sputum smear. A sputum smear can only detect pulmonary tuberculosis and is not always accurate, especially when it is performed by someone without enough training. Other tests may be costly, and can only target a certain number of patients. Most tests still require multiple visits to determine the results of the test. On the other hand, tests that are cheap and fast often are not very accurate.
Portable, Reliable, Fast and Cheap
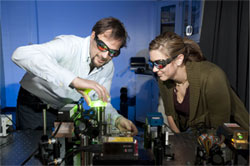
Dr. Diego Krapf and grad student Kristen Jevsevar align a fluorescence microscope.In order to truly identify everyone infected with M. tuberculosis bacteria and eliminate the disease, the test must be cheap, fast, portable, and accurate. Dr. Diego Krapf, Assistant Professor of Engineering at Colorado State University, and a team of engineers, physicists, chemists, and biologists, are working together to develop just such a diagnostic tool.
Dr. Krapf is using his background in optics and biophysics to develop a biosensor to accurately detect M. tuberculosis infection. He envisions a testing kit that would contain the materials for collecting samples and the portable electronic device that could read them all in a small box.
Grad student Aubrey Weigel aligns the fluorescence microscope.To understand the technology we first need to know more about the M. tuberculosis bacteria. The M. tuberculosis bacteria shed specific proteins when they die. These proteins are found in body fluids such as the blood, urine, or saliva, and can be used to identify the presence of M. tuberculosis. The biologists in Dr. Krapfs team are looking at two of these proteins known as antigen-85 and alpha-crystallin.
This technology would identify these proteins in a sample of body fluid:
This body fluid sample would first be mixed with fluorescent antibodies for the targeted proteins antigen-85 and alpha crystallin.
Any of these proteins present in the sample would bind to the fluorescent markers and thus be detectable by the sensor. The fluorescent fluid would then be inserted into a small channel between two glass slides that is coated with antibodies for the targeted proteins. The proteins and their fluorescent markers would bind to the antibodies and stick to the channel.
The chamber would then be rinsed with water to remove the rest of the proteins and other molecules in the fluid. In an ideal situation, only the targeted molecules and their fluorescent markers would be left on the slide.
Once prepared, the slide would be inserted into an electronic device to measure the presence of the targeted proteins based on their fluorescence. A large amount of these fluorescent proteins indicate a positive test for TB.
Technical Difficulties
Image from the microscope: each spot is an individual fluorescently labeled TB protein.
One problem with many similar tests is that other molecules, not just the targeted proteins, bind to the antibodies and create noise that makes detection difficult. Dr. Krapf and his team work with specialized surface chemistries that bind specifically to the targeted proteins, antigen-85 and alpha-crystallin. Researchers are also looking into other proteins that may be better indicators of the bacteria. They plan to use surfaces that bind only the targeted proteins and their fluorescent markers. This will create a very sensitive device and a reading could take only a couple of minutes.
The visualization of these molecules is very easy to do in the lab. A high-powered microscope on a heavy table can see even a single protein that has bound to the glass. This technology, however, is not portable, nor is it available in the poor, rural areas where it is most needed. As a result, the team is working to develop equally sensitive optics using cheap, everyday, portable materials. For example, instead of using expensive lasers, the technology employs commercial lasers, such as those found at the checkout counter in the supermarket. Unlike laboratory lasers, these lasers are mass produced and are very cheap. In order for this device to be portable, it cannot depend on high-powered machines. To that end, the researchers are developing electronics that will enable the device to be battery-run and only require low power. Dr. Krapf is currently experimenting with a device that would cost $200, compared to the $150,000 cost of the laboratory microscope.
Cost-Efficiency vs. Sensitivity
Dr. Krapf and his team of researchers are testing the limits of the sensitivity of the device. They are trying to reduce costs by using cheaper, commercially available materials, while at the same time increasing sensitivity. The aim is to optimize the trade-off between cost efficiency and sensitivity. The current experiments with the device use normal fluid samples that are then injected with the specific targeted proteins. In order to make this device really work in the field, the next step is to take quantitative measurements to determine how many molecules of the targeted proteins are present in the blood, urine, or saliva, of infected people. So there are many steps ahead before this device can be put to the true test on the ground in tuberculosis-infected areas. Dr. Krapf hopes that the use of the device will help reduce the burden of tuberculosis in developing countries by identifying populations with latent tuberculosis so they can be treated before spreading the infection to others. If successful, Dr. Krapf believes this biosensor technology could become a model for sensors for other infectious diseases.
The Krapf Laboratory from left to right: Dr. Diego Krapf, Kristen Jevsevar, Nathan Proper.
Dr. Diego Krapf is an Assistant Professor of Electrical and Computer Engineering and Bioengineering at Colorado State University. He has been interested in science from a very young age and really likes the mathematical applications of physics. He went to school in applied physics, working in the microelectronic industry with semiconductor devices
and nanotechnology
. He realized that rather than refining established techniques, he wanted to develop new technologies and contribute to humanity, so he moved to biophysics and biomedical applications. His latest project is the creation of a biosensor for the detection of tuberculosis. Dr. Krapf lives with his family near the Rocky Mountains and enjoys hiking, skiing, snowshoeing, and visiting the nearby national parks.
Research collaborators from the Colorado State University Department of Microbiology, Immunology and Pathology from left to right: Dr. Michael R. McNeil, Dr. John S. Spencer
For more information:
Girosi, F. et al. Developing and interpreting models to improve diagnostics in developing countries. 2006. Nature, Supplement 1: 3-8
Keeler, E. et al. Reducing the global burden of tuberculosis: the contribution of improved diagnostics. 2006. Nature, Supplement 1: 49-57.
Pai, M. and R. OBrien. New diagnostics for Latent and Active Tuberculosis: State of the Art and Future Prospects.2008. Seminars in Respiratory and Critical Care Medicine, 29(5): 560-568.
1.Smith, B.S., Krapf, D, et al. Fluorescence Immunoassay for the Detection of Latent Tuberculosis Antigens with Single Molecule Sensitivity 2009. in Frontiers in Optics 2009 (Optical Society of America), JWC 68
Moloch In this socially conscious, silent 1914 propaganda film, greed contributes to the spread of tuberculosis, with devastating effect on both the poor Swanson family and the wealthy Pratt family. http://www.youtube.com/watch?v=nOdQS93fp6I
This early 1960s Pathé newsreel tells the story of Glasgows program to x-ray 250,000 people in an effort to reduce the citys notoriously high TB rate. Newsreels like this were once common in movie theaters before the main feature. http://www.youtube.com/watch?v=21_ddVcx94s